A quick reference guide for diagnostic ECG criteria with examples. Will continue to update regularly.
P-Wave Abnormalities
Right atrial enlargement (RAE)
2 things help me remember RAE. First, the normal P-wave on an ECG typically represents the left atrium because the right atrium is typically smaller and it’s electrical current is typically hidden in the left atrium’s electrical signal. Second, the SA node sits in the right atrium. So when the right atrium gets enlarged we start to see it on the ECG. The P-wave gets BIGGER! I think of it similar to what we see in left ventricular hypertrophy. Typically, in a normal QRS complex we only see the left ventricle because it’s size and electrical signal is so much larger than the right atrium (similar to our atria). However, in LVH the left ventricle gets even larger. So the electrical signal it puts out is even bigger too. This is just like what happens in RAE. The right atrium is able to be seen in the P-wave which manifests with TALL P-waves. Thus, the diagnostic criterion are:
Inferior lead P-waves: >2.5 mm in height (tall positive P-wave because the SA node is superior in the heart so the electrical signal in the inferior leads, the direction the electrical impulse goes toward, will be larger in size)
>1.5mm in V1, V2
Clinically can be seen in RVH, COPD, pHTN > CHD >>tricuspid stenosis
Left atrial enlargement (LAE)
Back to our discussion about P-waves. In normal physiology the SA node in the right atrium fires and then the signal has to travel all the way over the left atrium. We already know that on normal ECG’s that the P-wave represents the left atrium. Thus, if the left atrium gets enlarged you will see LONGER P-waves because it will take more time for that signal to reach the entirety of the left atrium. Or at least that’s how I remember it in my head. Thus, for LAE think “1 box deep, 1 box wide”. If you can fit 1 small box inside the negatively deflected P-wave you should be thinking about LAE. The diagnostic criterion are:
Terminal portion V1 > 1mm deep, >40ms duration
Inferior leads: notched P-wave > 120ms
Biatrial enlargement (BAE)
You can also have both diagnostic criterion met for both left and right atrial enlargement. In these cases we simply call it biatrial enlargement. Here’s a quick and dirty reference for atrial enlargement:
Ventricular Hypertrophy
Left Ventricular Hypertrophy (LVH)
There are a LOT of criterion for LVH but the most frequent ones that I use in clinical practice are:
aVL >11 (Sokolow-Lyon ‘stand alone‘ criteria)
Cornell Criteria: R wave in avL + S wave in V3 > 28mm in men/> 20mm in women (Easy way to remember: CorneLL has 2 L’s, aVL has 1 L. Add them together to remember you use lead V3)
Sokolow-Lyon Criteria: S wave in V1 + R wave in V5 or V6 > 35mm
Delayed intrinsicoid deflection in V5, V6 >50ms (interestingly this is the only non-voltage criteria for LVH)
LVH can also have a ‘strain pattern’ with T-wave inversions (TWI) as seen in the ECG below.
LVH with strain pattern in I, II, V5, V6
Right Ventricular Hypertrophy (RVH)
RAD: mean QRS axis ≥ 100 degrees
Secondary ST-T segment changes (STD, TWI) in right precordial leads
(R/S ratio in V1 > R/S ratio in V5, V6) or (R/S ration in V6 <1) or (R wave > 7mm in V1)
Clinically, Posterior MI can mimic RVH
Factors that favor RVH diagnosis: concomitant RAD, TWI in V1-V2
Factors that favor posterior MI: presence of inferior Q-waves
Combined Ventricular Hypertrophy
Exists when criteria for both isoloated LVH) and RVH are met
Should be suspected when criteria for LVH is present but QRS axis is > 90 degrees or criteria for right atrial enlargement exist
R/S ratio approximately equal to 1 in both V3 and V4 (Kutz-Wachtel phenomenon)
Diagnosis: Atrial flutter, LAD, LVH, RVH, iRBBB
Intraventricular Conduction
Left Bundle Branch Block (LBBB)
QRS ≥120 ms
Terminal S-wave in V1 (late forces of QRS should be negative)
I, aVL, V5, V6: Broad notched or slurred R-wave. Occasional RS pattern in V5, V6 may be attributed to displaced transition of QRS complex)
No Q-waves in I, V5, V6 but in aVL a narrow Q-wave may be present without myocardial pathology
Delayed onset of intrinsicoid deflection >60 ms from beginning of QRS to peak of R-wave in V5, V6 but normal in V1-V3 when small initial R-wave can be discerned
Left Anterior Fascicular Block (LAFB)
LAD (QRS axis between -45 to -90 degrees) and mean QRS duration < 120 ms
qR complexes in I, aVL
rS complexes in II, III, aVF
Prolonged R wave peak time in aVL > 45ms (from beginning of QRS complex to peak of R wave)
*Absence of other causes of marked LAD such as inferior MI or LVH
Note: The entire left bundle conduction system of the heart is made up of two fascicles, one anterior and one posterior. The left anterior fascicle supplies fibers to the anterior and lateral walls of the left ventricle. The above criteria of left anterior fascicular block do not apply to patients with congenital heart disease in whom left-axis deviation is present in infancy.
Left Posterior Fascicular Block (LPFB)
RAD (QRS axis 90 to 180 degrees in adults) with mean QRS duration < 120 ms
rS complexes in leads I and aVL
qR complexes in leads II, III and aVF
*Absence of other causes of right axis deviation including lateral MI, dextrocardia, or RVH
Note: The entire left bundle conduction system of the heart is made up of two fascicles, one anterior and one posterior. The left posterior fascicle is shorter and thicker than the left anterior, and receives dual blood supply from both the left and right coronary arteries. Multivessel coronary artery disease is the most common cause of left posterior fascicular block.
Right Bundle Branch Block (RBBB)
QRS ≥ 120 ms
V1, V2: RSR’ with secondary R-wave usually wider than initial R-wave
Minority of patients may have a wide and often notched R wave pattern in lead V1 and/or V2
S wave duration > than R wave or > 40 ms in leads I and V6
Normal R peak time in leads V5 and V6 but > 50 ms in lead V1
Of the above criteria, the first 3 should be present to make the diagnosis. When a pure dominant R wave with or without a notch is present in V1, the 4th criteria should be satisfied
Incomplete Right Bundle Branch Block (iRBBB)
Same criteria for RBBB but QRS < 120ms but > 100ms
Non-specific inter-ventricular conduction delay
QRS ≥ 110 ms
Specific criteria for RBBB, LBBB not met
Quick and dirty reference to compare LBBB and RBBB:
Atrial Rhythms
Sinus Rhythm
In medical school we are taught this incorrectly. The correct way to tell that a P-wave is of sinus origin is that they are:
Upright in the inferior leads (remember the sinus node is in the right atrium so the electrical wave will go from the top down and thus be positive inferiorly)
Biphasic in V1
Axis between 0 to 75 degrees (i.e. upright in the inferior leads)
The number of P-waves before every QRS complex is irrelevant. You can have sinus rhythm but be in complete heart block. Or have sinus rhythm but have second degree type I or type II heart block. Generally however they should have the same morphology. A single P-wave with a different morphology can indicate a premature atrial complex (PAC) but if you have multiple different P-wave morphologies then you might be dealing with wandering atrial pacemaker (WAP) or multifocal atrial tachycardia (MAT). I think of WAP and MAT as the same rhythm across a spectrum ranging from a normal heart rate (WAP) to a fast heart rate (MAT).
Sinus Arrhythmia
Diagnostic criteria:
Normal P wave axis (0 to 75 degrees; i.e. upright in leads I and II)
P-P interval varies by > 10% or 0.16 seconds
tl;dr normal sinus P-waves (as above) but P-P interval varies by >10% or 160ms (4 little boxes). ECG intervals can vary with respiration but they shouldn’t vary by more than 10%. Often incidental without major clinical significance
I recently came back from a trip to Barbados where I gave the incoming first semester class of Ross University some advice on how to succeed in med school. Here’s a summary of my top med school blog posts broken up into various categories:
The most frequently asked question that I receive from students from around the world is ‘should I apply to a Caribbean medical school?’. There are plenty of blog posts on the internet that provide advise without objective evidence. So before I give you my unfiltered opinion I want to first present the cold hard facts surrounding the topic as well as some information that is not common knowledge to many pre-med students, most individuals outside of medicine, and future Caribbean graduates. My hope is to arm you with data so that you can make an informed decision about applying to Caribbean medical schools and how best to prepare yourself for success when attending a Caribbean medical school. Before jumping into the benefits and drawbacks of these programs let’s first take a step back and look at the journey of becoming a doctor in the United States.
Part I: Becoming a doctor in the United States
‘What do you call someone who graduates at the bottom of their class in medical school? Unemployed.‘
In order to apply to medical school in the United States you are required, at a minimum, to have completed your pre-med requisite courses which include one year of biology, one year of physics, one year of english, and two years of chemistry (usually general and organic chemistry). Many medical schools are also now requiring molecular genetics and biochemistry. For school specific requirements you can check out the Medical School Admission Requirement website. On top of your pre-med course requirements most American medical schools require a stellar MCAT score, extracurricular activities inside and outside of the medical field, and shadowing experiences of some sort. For the sake of brevity this blog post will not cover the lengthy topic of how to get into medical school.
There are two types of medical schools in the United States- allopathic and osteopathic. Students who graduate from allopathic medical schools earn an ‘M.D.’ which stands for ‘medical doctor‘ and students who graduate from osteopathic medical schools are a ‘D.O.‘ which stands for ‘doctor of osteopathic medicine’. There are differences between the two in certain aspects of their training and the standardized tests they have to take but in clinical practice they are quite synonymous and are otherwise both ‘doctors’ in every modern sense of the word.
In general, medical school in the United States is four years. This includes both MD and DO programs. However to make matters slightly more complicated there are also many medical schools that offer dual MD/PhD programs (generally speaking these are 7 year programs) as well some schools that offer or even require an additional year of research. Other medical schools also offer dual degrees. Some schools offer an MBA or MPH alongside their medical degree. So generally speaking medical school is a four year process but clearly there are exceptions to the rule if you choose to pursue a different path.
After graduating from medical school you are now a doctor, in name at least. In the United States you cannot practice medicine independently without completing residency training. This is worth repeating. In the United States you cannot practice medicine independently without completing residency training. This is the crux of issue regarding Caribbean medical schools. Acceptance into medical school ≠ a job. Acceptance into medical school guarantees you two fancy letters at the end of your name but without landing a residency position you will never practice medicine as a physician. In the remainder of this post I will explain that, based on prior residency match data and from personal experience, by attending a Caribbean medical school you put yourself at a distinct and intrinsic disadvantage in your ability to obtain a residency position in the United States compared with graduates from stateside MD and DO medical schools.
Part II: The Match
‘Like speed-dating but worse’
If we are going to understand why Caribbean medical graduates are at a disadvantage historically compared to American medical graduates we have to first understand the National Resident Matching Program (NRMP), or ‘the match’.
Near the end of the third year of medical school students begin applying for residency. The program known as ERAS, or the electronic residency application system, is the online application students use to apply. It is a common application that almost every residency program uses and makes applying for residency simpler. After uploading your application and appropriate paperwork all you have to do, generally speaking, is click which school you want to apply to.
After the application deadline passes residency programs begin downloading applications. Many programs have hard cut offs. For instance, some programs require you to have a step score above a certain value and if your score is not up to par then your application simply won’t be looked at. Next the residency program picks who to send interview invitations to. Interview season generally lasts 3-4 months from October to January but varies from specialty to specialty. After interview season concludes both students and programs must submit ‘rank lists’. Rank lists are exactly what they sound like. Applicants rank which programs, from the ones they interviewed with, that they want to go to with their most highly sought after program at number 1 and then rank each subsequent program down the line. Programs do the same with applicants. Eventually a computer system attempts to ‘match’ students and programs together to make the best possible fit based on each respective applicant and programs choices. The following video is the best one that I could find that explains this quite complex process as succinctly as possible.
On the Monday of ‘match week’ applicants find out if they have matched or not. They find out where they matched on Friday. The reason for this is that if a student does not match they can participate in the SOAP, or supplemental offer and acceptance program. This is a second chance to try and match into a residency position that went unfilled. More information on the SOAP can be seen at The NRMP website.
This is why medical students ‘match’ into residency spots. It isn’t as simple as a job application. And Caribbean medical students match into residency at a far lower rate compared to their stateside colleagues.
Chapter 3: Raw Data
‘Without data you’re just another person with an opinion’
So now that we kind of understand what it means to ‘match’ into residency let’s finally take a look at the raw data from the 2018 main residency match. The NRMP data is widely available and I encourage you to take a look yourself here. The data describes Caribbean graduates with the term ‘international medical graduates’ or an ‘IMG’. These are further split into two categories: US citizen IMG and non-US citizen IMG. So if you are a US citizen and went to a Caribbean medical school then you are considered a US IMG.
In 2018 there were 37,103 active applicants and 30,232 first year and 2,935 second year residency positions. The following are the match rates for each type of applicant:
US allopathic graduates (MD’s): 94.3%
US osteopathic graduates (DO’s): 81.7%
US IMG: 57.1%
Non-US IMG: 56.1%
If you only remember one thing from this post then this should be it. Only 57.1% of US IMG’s, or people like me who are US citizen Caribbean medical graduates, match into residency positions versus 94.3% of US allopathic grads and 81.7% of US osteopathic grads. This is terrifying! Imaging going through four years of medical school, accumulate a crushing amount of debt, only to end up without a job or the ability to practice as a physician (check out prior interview posts with individuals who went through that exact experience).
An interesting graph from the NRMP data shows that not every specialty ranks equally.
This graphic shows that the specialty in which the highest percentage of US IMG’s were able to match into was pediatrics at 69.8% of applicants matching while psychiatry on the other hand was the most difficult specialty for US IMG’s to match into at 30%.
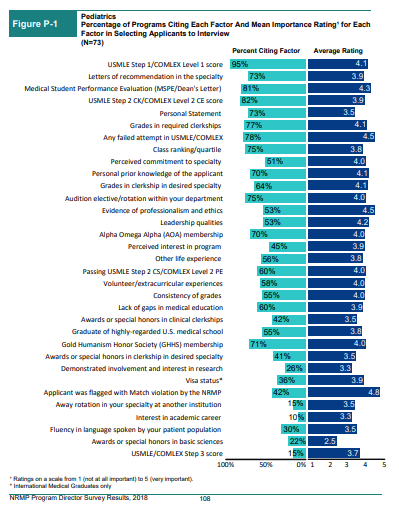
So why do Caribbean graduates have a greater difficulty matching? Let’s take a look at NRMP data from a survey of program directors. This survey is also widely available and I encourage you to analyze it yourself here. The survey was sent to 209 program directors (PD’s) and 78 responded, or 37.3%.
The data shows each individual factor that program directors find important when they choose applicants to interview and rank for residency. As you can see below the USMLE step 1 score, based on this data, is by far the most important factor for choosing applicants to interview.
So a strong STEP 1 or COMLEX 1 score gets your foot in the door but it does not necessarily get you the job. Now let’s use the data from pediatric program directors (PD’s) for the next few graphs. This next graph shows the most important factors that pediatric PD’s felt were the most important factors when ranking applicants.
This graph clearly shows that the more important component of how medical students are ranked on a program’s rank order list is how an applicant interacts with residents and faculty on interview day. Again, a strong USMLE step 1 score seems to be of critical importance in helping get an applicant’s foot in the door but how they interacted on interview day earns medical students the opportunity to walk through it. Of note, each specialty seems to vary slightly in what they rank as most to least important but grossly these trends seem consistent across the board.
The issue however is that getting a stellar USMLE step 1 score isn’t the only obstacle when it comes to matching into residency for Caribbean medical students. At the end of the day all medical students learn the same science but not all medical students have access to the same residency programs.
The same survey of pediatric PD’s (and the same specialty that in 2018 had the highest successful match rate from US IMG’s) shows that some program’s won’t even consider an applicant if they graduated from a Caribbean medical school. The graph below shows that out of the PD’s who responded to the survey only 67% of them typically even interview US IMG’s.
Broken down even more we see that an even smaller percentage of programs will ‘often’ interview and rank candidates from Caribbean medical schools. This is another huge point that you should take away from this blog post.
Again, the match rate for US IMG’s in 2018 was 57.1% versus 94.3% and 81.7% match rate for allopathic and osteopathic grads respectively. I believe that part of that intrinsic disadvantage is that some residency programs simply won’t touch Caribbean medical school graduates. You simply can’t get a job if they won’t interview you for it.
Another unfortunate aspect of being a Caribbean graduate is that it seems to impact the fellowship match too, although to a lesser degree compared to the residency match. If we take a look at the results of the 2019 fellowship match data we can see a clear trend that does not favor Caribbean graduates. The following are the match rates for fellowships in 2019:
US allopathic graduates (MD’s): 89.4%
US osteopathic graduates (DO’s): 78.9%
US IMG: 68.5%
Non-US IMG: 71.4%
For the sake of brevity I won’t delve too much into this data because the fellowship match is a little bit more complicated and not so clear cut. I’m not certain as to why Caribbean medical graduates have a tougher time matching into fellowships but I am certain that some fellowship programs won’t touch a Caribbean graduate just like how some residency programs don’t.
Chapter 4: Informed Consent
‘Without consent surgery would be considered assault’
In medicine before we perform any test or procedure we are required to get informed consent from our patient. Informed consent is the concept of understanding all of the possible consequences with full knowledge of the possible risks and benefits of said procedure. I think the same should be true about applying to Caribbean medical schools and after getting through all of that data I think we’re closer to fully understanding the implications of attending a Caribbean medical school.
Don’t get me wrong, I’m not trying to scare you away from applying. I graduated from a Caribbean medical school, matched into an internal medicine residency program, and successfully matched into a cardiovascular disease fellowship. There are plenty of success stories that originate in the Caribbean and I’ve interviewed nearly a dozen of my colleagues who matched into competitive specialties like emergency medicine and surgery. But Caribbean medical schools aren’t for everyone and you should understand that before you sign up or apply.
Chapter 5: The Caribbean Stigma
‘Some stereotypes originate in truth but are exaggerated by myth’
There is a common misconception in the pre-med community about the ‘Caribbean stigma’. This myth that there would be a doctor or nurse in the hospital you are rotating in that would choose not to work with you because of where you went to medical school. Or that Caribbean medical students are not as qualified as their stateside counterparts. Unfortunately the stigma is steeped in truth.
Caribbean medical students go to the Caribbean because they could not get into a US MD or DO program. That’s why I went to Ross University. I applied to 36 medical schools and Ross University was the only one that accepted me. Caribbean medical schools typically have lower standards and thus not every medical student makes it to graduation. I could not find the statistics on the attrition rate from stateside or Caribbean medical schools but I can speak from experience.
Out of the 440 students who started with me in my first semester of medical school only 76% advanced to their second semester. Although this is only one anecdotal piece of evidence and shouldn’t be used to grossly generalize against all Caribbean schools it does in fact happen. Furthermore, the fact that some Caribbean medical schools are for profit organizations is worrying to me and further underlines the fact that they accept too many students who otherwise wouldn’t be accepted into stateside medical schools. Not to mention that medical school in the Caribbean is just as expensive as medical school in the US. So if you are unable to secure a residency position you will be left with massive loans and a hard road ahead to paying them off.
So although the ‘Caribbean stigma’ exists when applying to and while attending medical school once you make to the hospital nobody cares where you went to med school. In the hospital I’ve met incredibly passionate, intelligent, and competent medical students, residents, fellows, and attending physicians from both Caribbean and allopathic and osteopathic medical schools. I’ve also met terribly incompetent individuals from Caribbean, allopathic, osteopathic medical schools too. Just because you attended a certain medical school doesn’t make you a better or worse doctor. Sure, it certainly impacts your ability to match into residency but there isn’t a single nurse, physician assistant, or doctor out there who will treat you any better or worse just because of what med school you went to.
Chapter 6: The Life of a Caribbean Medical Student
‘It doesn’t really matter where go to medical school because it’s always 72 and fluorescent in the library’
The ‘big four’ Caribbean medical schools are:
St. George’s University (SGU)
Ross University
American University of the Caribbean
Saba University
I won’t delve into the specifics of each individual Caribbean medical school and this list is not exhaustive but each of these schools share many similarities with the majority of Caribbean medical schools. In general when you go to a Caribbean med school only the first two years are spent ‘on the island’, or in the actual Caribbean. These first two years are spent in the traditional classroom where we are taught the same basic sciences that allopathic and osteopathic med students learn in preparation for USMLE step 1. It’s really not that bad. I enjoyed my time on the island. I remember being stressed out before my first major exam so I took a stroll on the beach to relax. After leaving the island most medical students rotate in hospitals across the US that each respective medical school has affiliations with. I rotated in hospitals in New York and Florida.
Chapter 7: The End Game
Measure twice, cut once
Your first choice should be to get into a US allopathic or osteopathic program. People who are not accepted at first often work on improving their weak spots in their resumé or work while they study to retake the MCAT. Often students will work a few years, do research, get various master’s degrees, or do a post-baccalaureate degree. Others, like me, don’t want to wait and choose to attend a Caribbean medical school instead.
This is a viable option for certain students but it might not be the right fit for everyone. Some residency specialties, like neurosurgery, orthopedic surgery, ophthalmology, otolaryngology, plastic surgery, urology, and dermatology, are some of the most competitive medical specialties that exist. Even US graduates often have difficultly earning these residency positions (my osteopathic colleague took three attempts to match into derm and he was a PhD too!). By attending a Caribbean medical school you are again giving yourself another uphill battle to fight. So if your heart is truly set on one of these specialties understand that although it is not impossible to match as a US IMG it will make it increasingly more difficult to do so. That being said, if you know you want to go into primary care fields like internal medicine, family medicine, or pediatrics then a Caribbean medical school might be the right fit for you. Again many residency, and fellowship, programs simply won’t look at you because you are a US IMG. So you might not be able to go to an ivy league internal medicine residency or fellowship program but you certainly can still become a doctor.
The ironic part of all of this is that in order to be a good doctor at the end of the day it really doesn’t matter where you went to medical school or what you got on your USMLE step 1 (as this blog post points out). In residency nobody care what your test scores were and when you are an attending your patients won’t care that you went to an ivy league school if you aren’t compassionate, kind, caring, or intelligent. And yet if you don’t do well on your exams, especially coming from the Caribbean, you hurt your chances of ever being able to treat future patients. Whether you like it or not this is the current status quo. So if you go to the Caribbean be ready to work hard, crush your step exams, and get great letters of recommendation.
I hope this post helped uncover some of the hidden curriculum of medical school and residency and didn’t scare you away from applying to Caribbean medical schools. Ross University was the only medical school I was accepted to and they gave me the opportunity to pursue my dream of becoming a physician. It’s up to you to make the best decision for your future career and then make the most of that opportunity. Hopefully now you can do so with confidence and informed consent.
You can also check out my YouTube video on the topic below:
Drop me any follow up questions that you may have below and be sure to subscribe so you don’t miss my next post!
One of the most frequently asked questions that I receive from medical students is about how to prepare for their first year of resident. It parallels one of the most common fears among medical students in that they will not be adequately prepared for day one of residency. It’s a valid concern because you will never truly be ready for intern year but if you’ve made it this far in your training then you are likely ready enough. Almost everything you learn intern year isn’t taught in medical school because you have to do actively do it to learn it. At least that’s what I thought until I came across OnlineMedEd.. It’s the only resource I’ve found that actually prepares medical students reasonably well for intern year. Again, nothing is going to make you fully prepared but this is as close as you’re gonna get.
I started using OnlineMedEd during third year of medical school
OnlineMedEd is an amazing resource with videos that help explain complicated topics that overlap real world experience with the textbook. They do an amazing job of translating all of that USMLE step 1 material into actual practical knowledge so you can look sharp on all of your third year rotations. I would watch a few before each rotation started and it showed. Dustin and the OnlineMedEd team also drill home all of the important facts that are frequently tested on step 2 CK. Sure, nothing will ever replace UWorld but OnlineMedEd gives it a run for it’s money. Start using OME early and often.
A curriculum for fourth year medical students
Your fourth year of medical school is a magical time especially after interview season is over and your rank list is finalized. You’re basically just waiting to graduate and planning your vacation to South East Asia. It is all to easy to fall into a trap of laziness and forget that you are going to be a full fledged doctor in 6 short months (well technically you’ll be an intern but a doctor nonetheless). If you dedicate yourself to the structure of OnlineMedEd during your fourth year you will have a dedicated curriculum that keeps you fresh and sharp on the wards. Sure, you’re still gonna forget a lot before intern year starts but at least OnlineMedEd will get you into some good habits.
It prepares you for intern year
My advise to all of my fourth year medical student is always the same- go home because life is too short to be spent in the hospital watching me type notes and at least one of us should see the sun today. I also tell them that the best way to be a good intern is to develop good habits while you are still in medical school. The dirty truth about residency is that you don’t need to be all that intelligent to be a good intern. You simply need to be efficient, thorough, and work hard. The sooner you develop habits that enable you to work smarter, and not harder, the better off you will be. OnlineMedEd has developed a fantastic Intern Boot Camp that helps you do exactly that. If I could do my fourth year all over again I would use the Intern Boot Camp and test out what does and does not work for me while I was still on the wards in the hospital. That way when I show up day one of residency I at least had a system that I knew worked for me. It’s like when I had to learn how to actually study in medical school- I wish I didn’t have to go through the process of figuring out what works best for me. I wish I knew how to study more efficiently back in undergrad. Likewise, take the time to learn the ropes of what it takes to be an intern while you are still a medical student.
Start studying for step 3
Ugh I know. Sorry for bringing up the USMLE’s again but you have to get it over with eventually. I’ve written extensively about when you should take USMLE Step 3 as well as how to study for USMLE step 3.If you use OnlineMedEd during your fourth year of medical school you will get a head start on it. You don’t need to use OnlineMedEd as your primary study aid but it will certainly help cement concepts in your head and make it easier for you once you start your dedicated step 3 study period as you transition from medical student to resident.
They also have great study products
Last thing I’ll mention are their study aides. The Intern Guide Book and the Quick Tables Book are great study tools for medical students. They succinctly provide you with a ton of well organized material. You have to fill in the blanks and annotate it just like any guide book. But if you are going to use OnlineMedEd then these books are essential as they go hand in hand with some of the videos. Just like any resource, the more you use it the more results you get from it!
So if you are interested in using OnlineMedEd check them out here: OnlineMedEd.
*Full disclosure: sponsored content. That being said, I only support brands that I believe in.*
One of the most frustrating aspects of medical school and residency is the hidden curriculum. The stuff you kind of just figure out along the way and wish you knew from the beginning. One part of the hidden curriculum of medical school and residency is research. Here are my tips on how to successfully get published.
First off, why bother doing research?
If you are a medical student it will make you stand out when applying to residency and if you are a resident applying for certain fellowships it might as well be mandatory. So the first reason is for your resumé. The second reason is that research forces you to learn a topic more extensively than you normally would otherwise. That’s my favorite reason to get involved in research. You end up learning so much more compared to just reading topics and doing practice questions. Additionally, you also learn to
Find a topic or field that interests you
The only thing worse than doing research is doing research on a topic or in a field that bores you. That’s why all of my research is in cardiology. So find a research project in a medical specialty or disease process that you find interesting.
Find a mentor
Okay, so I’ve sold you on the idea of doing research. Next, you found a field that interests you. But how do you just start a research project? The best way to approach finding a research project is approaching someone who is already doing research in that field or specialty. As a medical student, I asked the cardiologist I was working with if he knew of any interesting research going on in the cardiology department. He put me in touch with the right people who pointed me in the right direction. Ultimately, I got two publications out of the experience and learned a lot about cardiac magnetic resonance imaging.
Fast forward to residency and some of the best advise I’ve received has been from my senior residents and fellows. These are people who have already done what you want to accomplish. They are probably the most valuable resources you’ve got so use them! Better yet, get involved in their research projects to get your feet wet.
Additionally, don’t forget your co-residents or medical students. Some of my close friends and colleagues are doing amazing research and their tenacity to publish their work inspires me to get on my grind. They are another valuable resource. Some of my colleagues who already have a few research projects under their belt know the system and how to maneuver it. So don’t be shy or too proud and ask your successful colleagues how they did it.
Be curious
If you don’t understand something then ask! Be curious about medicine and uncover the reasoning behind clinical decision making. As much as we know about the human body there is still so much that we don’t understand and your questions on rounds one day might be the beginning of your research project.
What did I miss? What tips do you have to help medical students and residents get published? Comment below and don’t forget to subscribe so you don’t miss my next blog post!
At my hospital, we call first year residents ‘interns’ and all of the second and third year residents are the ‘senior residents’. It makes it easier for everyone in the hospital when you introduce yourself as ‘the intern’ or ‘the resident’. It set’s different expectations right from the get go. The biggest difference I’ve noticed between an intern and a resident is the following:
Now take a step back all the way to medical school where you don’t even know what you don’t know. It’s absolutely terrifying. You finish two years of classroom lectures and two years of clinical rotations and are eventually given a degree that essentially says ‘I know enough medical stuff to not kill someone’. And then on day one of residency you’re given 10 patients and realize they didn’t teach you any of this stuff in medical school. And that’s normal and okay. I still barely know what I’m doing everyday (I know, not really what you want to hear from your doctor).
My point that I’m trying to make to any medical student or intern reading this is that residency is terrifying at times and you won’t be okay. For some reason people don’t acknowledge this fact. That you are going to freak out at some point along the way either from anger, anxiety, fear, or all of the above. Just know that it’s going to get better.
I remember my first rapid response. A patient was in new onset atrial fibrillation with rapid ventricular response with a heart rate in the 180’s. He was hemodynamically unstable with oxygen saturation dropping into the low 80’s in front of my eyes. I arrived to the patient’s room and there’s one nurse getting a new EKG, another two nurses placing a new IV and drawing labs and an arterial blood gas, another nurse helping the respiratory therapist adjust the ventilator settings, as well as the rest of the floor nurses gathered outside the patient’s room to witness what was going on. “Oh good, the resident is here!” one nurse exclaimed. And then all of a sudden everyone turned and looked at me for guidance. Oh, and did I mention that this was the first time I had ever met this patient before? I was just covering overnight.
Thankfully this situation happened later on in the year so I was comfortable handling it. Not to mention I love being the center of attention and hearing the sound of my own voice so I live for these kind of moments. Ultimately the patient did fine and we resolved the underlying issue (mucous plugging caused hypoxia which induced a.fib which caused hypotension and altered mental status so regular deep suctioning would prevent this in the future).
Looking back at that rapid response, I would never have felt ready to handle that type of situation if you asked me during my first few months of residency. Even halfway through intern year I still would not have been nearly as confident in my medical knowledge or even in my ability to handle the stress of the situation. It is normal to be overwhelmed. You are only one month into residency. We don’t expect you to be full fledged attending physicians yet (again, I’m still figuring stuff out on the fly half the time). Just promise yourself to be better tomorrow than you were today. At the end of the day that’s all we can ask for. Micro improvements each and every day.
It’s been awhile since I used Picmonic. It was my go to medical school resource when I was a first and second-year med student and was even more valuable while I was studying for USMLE step 1 and step 2 CK. The more I used it, the more valuable it became. It is still to this day one of my three favorite medical school resources, which is why I was so excited to team up with Picmonic to help spread the word!
Picmonic is an online app that helps make studying easier, more efficient, and a little bit more fun. Let’s face it; medical school challenges you with a relentless barrage of information that requires absolute dedication to memorizing. And the worst part about studying in medical school is a simple fact that some stuff doesn’t make sense. You just have to memorize it. I’m talking about subjects like biochemistry, nutritional deficiencies, pharmacology, and microbiology. That’s why Picmonic is so amazing. It uses vivid pictures, stories, and wordplay to get all of that expensive medical school facts that you just have to know into your brain!
Let me just show you what I’m talking about
Each subject has a unique Picmonic ‘card’ that uses visual storytelling and pictures as mnemonics to help you remember more. They’re even better than flashcards! This is the Picmonic card for erythema nodosum, and I still remember it and use it to this day during residency. Inevitably during morning report, noon conference, patient presentations, or when I’m teaching my medical students this subject pops up. And my co-residents are just as shocked as my friends in medical school were when I rattle off the disease associated with erythema nodosum, represented by the Nodosaur with red bumps on its legs.
What I also love about Picmonic is that its cast of characters stays consistent throughout the Picmonic universe. For instance, take a look at the erythema nodosum card again down below. You’ll see a ‘cock (rooster) at sea’ representing coccidiomycosis circled in red.
Now check out the card for coccidioidomycosis. It’s the same rooster at sea, again circled in red.
Now take a second look at the coccidiomycosis card, but this time check out the granny-llama representing granulomatous inflammation, circled in yellow below. Now check out the same granny-llama circled in yellow on the Picmonic card for granulomatosis with polyangiitis (Wegeners).
And again, we see the same granny-llama representing granulomatous inflammation on the card for granulomatosis with polyangiitis (Wegeners).
Buy Picmonic Now!
Ultimately, I wholeheartedly believe that Picmonic helped me pass and succeed in medical school and helped me ace USMLE Step 1 and USMLE Step 2 CK (and even bails me out every once in awhile during residency). The more esoteric and difficult to memorize a subject is the more Picmonic flexes its muscles.
So if you’re tired of reading about Picmonic and ready to try it out, here is what you should do:
I’ve written a lot about the philosophy behind surviving and thriving in residency. Which is great and all but it doesn’t help you when you forgot to charge your phone last night and you’re already operating at 20% battery. Here’s what I use on a day-to-day basis as an internal medicine resident as well as what I keep in my white coat (or hidden somewhere on the floor) to make my day to day-to-day life easier (and fully charged).
What to do before starting medical school is one of the most commonly asked questions I hear from students about to begin their first semester of medical school. It’s the same question that I wrangled with after graduating medical school before starting my internal medicine residency. Here are my top three things to do with your last remaining days of freedom before starting medical school or residency.
Travel
Before starting residency I explored Thailand for two weeks and my only regret is that I didn’t stay longer. Traveling is a source of sustenance for the soul that can never truly be satiated. Traveling pushes you out of your comfort zone and forces you to grow as a person. You learn a lot about yourself when you remove your familiarities and submerge yourself in another culture and society. Who knows what a few weeks in another country will do for you. Go get lost so you can find yourself.
Nothing
As a resident we average one day off per week each month. That means we get, at minimum, four days off per month and sometimes that’s exactly what you get. So during residency, when you finally have free time on your hands you are often forced to be productive despite your zeal to just stay in bed and sleep all day. You have groceries to buy, laundry to fold, and an apartment to clean. Not to mention that research project you’re working on because you want to go into a competitive specialty. The work never stops. And after medical school you think your days of studying are over but step 3 and your specialty specific board exams always loom in the background. So if you want to sit and do nothing before you start medical school or residency then go sit and do nothing. You earned it and you don’t have to explain yourself to anyone.
Work
Med school is expensive and residency doesn’t pay too well so it certainly won’t hurt if you can muster up some extra cash while you can. I worked as the most overqualified AP bio tutor prior to starting residency. A friend of mine worked at our medical school as a standardized patient. A colleague of mine worked as a scribe in the emergency department. There are opportunities out there if you seek them out. Ultimately everyone’s financial and social situations are unique and you may not have the luxury to choose to work or not, let alone go on a vacation. For instance, the extra money I earned prior to residency helped me pay for my vacation while my friend who was a standardized patient used his money that he earned to pay for step 3 while my colleague used his extra money to pay for his kid’s braces. So work if you can but don’t overdo it. You don’t want to squander these last few weeks of sanity and freedom if you can afford to.
Take USMLE Step 3
Okay this is residency specific and should only be performed if you have so much extra time on your hands that you can do the aforementioned (1) Travel, (2) Nothing, and (3) Work and then still have more free time before starting residency. I would not advise anyone to take step 3 in lieu of traveling or doing absolutely nothing. Step 3 isn’t a particularly difficult test in my opinion. However, it is difficult to find the time and energy to study for it during residency. So do yourself a favor and if you have the time and money to take step 3 then register for the test, finish UWorld, and take it already (more detailed post on how to prepare for step 3 and when to take it is in the works).
What did you do the summer before medical school or residency?
July 1st marks the beginning of intern year for residents but they aren’t the only new faces in the hospital. The summer months are also the perfect time for premed undergrad students to get into the hospital for summer shadowing experiences. Shadowing experience gives premed students valuable clinical experience. Not to mention it’s essential to any medical school application. You probably have heard this before, or at least I hope you have, but in case you haven’t here’s how you can get the most out of your shadowing experience in the hospital.
Pursue what interests you, be curious, and ask questions
There’s nothing more refreshing than a young mind excited to learn. Your vigor makes it fun to work with you and a positive attitude makes me want to teach you more. You need to help me help you learn by actively asking questions so that we can direct your learning experience. It also further shows that you are actually interested in the field of medicine. So screw the cat- be curious and ask questions.
Put away your phone
Like it or not, people assume you are texting when you are on your phone. I’ve been victim to nurse technicians and attending physicians reprimanding me for ‘being on my phone’ even though I was actually researching information pertinent to our patient. Many people don’t mind when you quickly Google pertinent topics but rather play it safe than sorry. As a guideline keep your phone in your pocket and instead carry a small pen and pad with you in the hospital. Write down what you don’t know and Google it when you go home.
Don’t fall asleep
It happens by accident more often than you think. You finally get to sit down on a comfy couch after a long day on your feet in a comfortably warm room. Someone starts lecturing and their voice soothes you into slumber (Its like they want you to fall asleep!). Fight the urge and stay awake.
Look the part
You don’t need to wear a suit and tie but you should look presentable. When in doubt always overdress than underdress. You can always loosen a tie or take off a jacket but it’s hard to cover up your sneakers. In general, don’t look like you just woke up. At least put a comb through your hair before you show up. These are common sense things but it seems that common sense isn’t so common.
Be respectful
Medicine is an intimate art. People discuss things about themselves that they don’t tell anyone else or things that most people just straight up don’t want to know. So remember to treat your patient with respect and dignity regardless if you’re talking about their bowel movements or their cancer regiment.
Find a mentor
Much of what I just mentioned is about how you are perceived by your patients and the doctor you are shadowing. Instead of trying to conform to how others want you to act you should set your own standard that you hold yourself against. The best way to do this is to find a mentor who you want to be like when you’re a doctor. I’ve found several. I look up to an ICU/trauma surgeon who is able to apply mechanistic knowledge of disease processes to treat his patients, a cardiologist able to diagnose diseases with the use of his hands and stethoscope alone, and countless other individuals whose personal attributes I have grown to value. These attributes, like having a vast knowledge of medicine and the ability to apply that knowledge, won’t last unless you want them to. They are life long personality traits that you have to start developing now. So find someone who motivates you to be a better you and start the process towards becoming a physician today.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.